
Lessons from our Pupils: A Reflection [Episode 4]
In last week’s episode, Jay was joined by Dr. Yoshi Yonekawa and Dr. Will Parke for Journal Club. The three publications discussed involved pediatric retinal detachment surgery, open label extension of RISE and RIDE, and blood pressure fluctuations during intravitreal injections.
One of the articles discussed during Journal Club centered around the treatment for diabetic retinopathy. Diabetes is one of the most common chronic diseases in the United States, with the CDC estimating that more than 100 million people in the US have either diabetes or prediabetes. Currently, it is expected that 2 out of 5 Americans will develop type 2 diabetes in their lifetime. This disease carries the risk of many complications, including vision loss, neuropathy, nephropathy, skin problems and more. Importantly, it is the leading cause of vision loss in patients between 25 and 74 years of age. Because of the great global burden of diabetes and its impact on vision loss, in this post we wanted to review the classifications of diabetic retinopathy, and how the use of a monoclonal antibody can aid in treatment of this condition.
Diabetic retinopathy is the most common microvascular complication of diabetes and it is classified into either nonproliferative or proliferative subtypes. Nonproliferative DR represents the first visible changes seen in the retina due to diabetes. In this stage microaneurysms begin to appear as well as dot intraretinal hemorrhages, and retinal ischemia or infarction represented by “cotton wool” spots. Proliferative DR represents the end stage in the natural history of DR and presents with angiogenesis, or the formation of new blood vessels. In this stage there is severe hypoxia that stimulates the production of angiogenic factors, including VEGF.
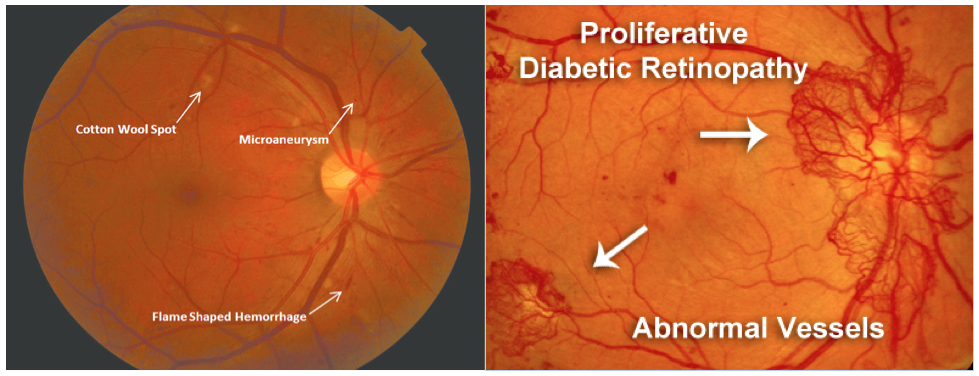
(Left) Image Credit: https://www.researchgate.net/figure/Moderate-non-proliferative-diabetic-retinopathy-with-no-diabetic-macular-edema_fig2_310612920
(Right) Image Credit: http://retinavitreous.com/diseases/dm_pdr.php
The RIDE and RISE Studies are long-term clinical studies looking at the use of Ranibizumab, a monoclonal antibody fragment, to treat proliferative diabetic retinopathy. This monoclonal antibody is designed to inhibit VEGF and prevent angiogenesis. VEGF, or Vascular Endothelial Growth Factor, is a protein produced by cells that stimulates the formation of blood vessels and endothelial cell growth, and causes the breakdown of the blood-retinal barrier. The state of severe hypoxia seen in proliferative DR induces the production of this molecule, which leads to retinal neovascularization. These new blood vessels are fragile, prone to bleeding, and can grow into the vitreous body. Thus, sight-affecting complications include vitreous hemorrhage and tractional retinal detachment. Monoclonal antibodies like Ranibizumab have been developed to prevent this progression by inhibiting VEGF.
An antibody molecule consists of four different polypeptide chains that join together to form a “Y” shape. Each antibody consists of two identical heavy chains and two identical light chains. Both polypeptides have a constant region and a variable region, and it is this variable region that binds to an antigen. A monoclonal antibody fragment, like the one used in the RIDE and RISE studies, only contains the antigen-binding fragment (Fab region) which is composed of both a heavy and a light chain with constant and variable regions. The loss of the Fc region makes this monoclonal antibody smaller allowing it to penetrate the retina more easily. Once in the retina, this antibody can bind to and inhibit VEGF, which prevents the molecule from binding to its receptor and thus helps to limit the progression of proliferative DR.
-Amy Kloosterboer

(Left) Image Credit: https://bxcell.com/antibody-structure/
(Right) Image Credit: https://www.scoop.it/t/victrelis-boceprevir-merck-fda-review-approval/p/4069081506/2016/09/13/scfv-fab-construction-and-purification-fab-creative-biolabs